
Jessica Moorhouse, author and Certified Financial Counsellor, focuses on wallets and well-being and what happens when they collide.
In recent years, there has been a global pandemic, rising costs of living, stagnating wages, geopolitical uncertainty, and tariffs, to name a few things. “We’ve been consistently talking about inconsistency since 2020,” Moorhouse notes, saying that millennials, in particular, are primed to wonder when the next big global shift is going to hit them.
For Gen Z, these experiences are baked in, and they have an extensive associated vocabulary, Moorhouse says. Consider the term “Menty B,” used widely on social media. “This is freaky to have shorthand slang for a mental breakdown,” she says. “That’s a concern – that it’s just normal to have anxiety, or to not be able to get up in the morning. There is a sense that you’re supposed to laugh it off, make a TikTok, and go to work.”
It carries a sense of solidarity among a generation struggling with financial disillusionment. They believe the system is broken because wages are not keeping up with the cost of living, and housing prices are too high.
It’s a heavy burden. Research indicates that economic conditions and related factors, including unemployment and poverty, can significantly impact suicide rates. Moorhouse highlights a study from the UK-based Money and Mental Health Policy Institute, which shows that 46 percent of people in debt have a mental health issue, and 86 percent of survey participants said their financial situation worsened their mental health problems and led to increased stress and anxiety. Likewise, 18 percent of individuals with mental health issues fall into debt, with 72 percent reporting that their mental health problems worsened their financial situation, creating a never-ending cycle.
Serena Dawson (a pseudonym), 19, observes some of these issues within her social circle. She lives in a major city in Ontario and is taking a gap year while working multiple jobs. She and many of her friends consider retirement a myth because of the astronomical cost of living and wages that don’t cover shelter expenses in nearly every city in Canada; they feel that policymakers are unaware of how to reform the system to benefit young people.
“Most young adults have at least three jobs, and I know people with up to six jobs,” she says. “One job doesn’t provide enough to meet basic needs, so people supplement with additional part-time jobs, contract work, and operating side hustles such as baking businesses out of their homes.”
Working all the time with competing commitments leaves little time for socializing or sleep, she says. “The toll on mental health is heavy. Conversations about anxiety, depression, and chronic health issues are everyday occurrences.”
Hustle, anxiety, repeat
The usual antidote to economic woes has traditionally been self-improvement. However, for many, traditional paths to advancement — like higher education — no longer feel worthwhile. Degrees don’t always guarantee jobs or stability, raising doubts about whether the investment pays off.
This confluence of conditions is something seemingly distinct to Generation Z. Psychology Today characterized this generation’s grief as one about unattainable developmental milestones, such as starting a family, owning a home, or retiring with financial stability.
“The disappearance of additional cultural anchor points, such as affordable education, a shared sense of truth, and community cohesion, only deepens the distress.”
For millennials, there was a different framing of their challenges with putting bread on the table.
“It was annoying to see the characterization that we’re lazy, avocado-toast-over spenders,” Moorhouse says. “We have three jobs! If we weren’t going to figure it out, we wouldn’t have three jobs – we would just give up.”
In this regard, traditional financial advice falls flat. This generation and those that follow are inheriting a different set of rules than their parents or grandparents did.
“Boomers, especially, did have a lot of privilege and gains on their homes,” Moorhouse notes, “and they took it as a baseline – as if everyone can afford a house or get a job at an executive level without advanced degrees. There was a big shift after that generation. You just can’t get that anymore.”
From debt to despair and back again – rethinking financial advice
The idea for this series grew out of young people’s perspectives—those finishing high school, launching careers, or trying to find footing in a shifting economy. Their common refrain: financial dystopia and distress. Stable jobs, home ownership, and retirement feel out of reach, with early setbacks snowballing into lifelong hurdles. Economists call this “scarring.” We ask: What are the mental health impacts, and what policy shifts are needed?
Whether you view artificial intelligence as an opportunity or an extinction event, its propulsion marks an inflection point in our society, and its impacts on the job market are playing out in real time. How do we build resilience—personally and collectively—while weaving psychological health and safety into economic policy?
As the world changes, what advice and tips do we need now? How can financial literacy be connected to emotional awareness as linked concepts? We ask practitioners and people with lived experience for their strategies.
Watch for the entire series published in October and November 2025 for Financial Literacy Month in The Catalyst, the magazine of the Mental Health Commission of Canada. Follow us on LinkedIn to see new articles and resources.
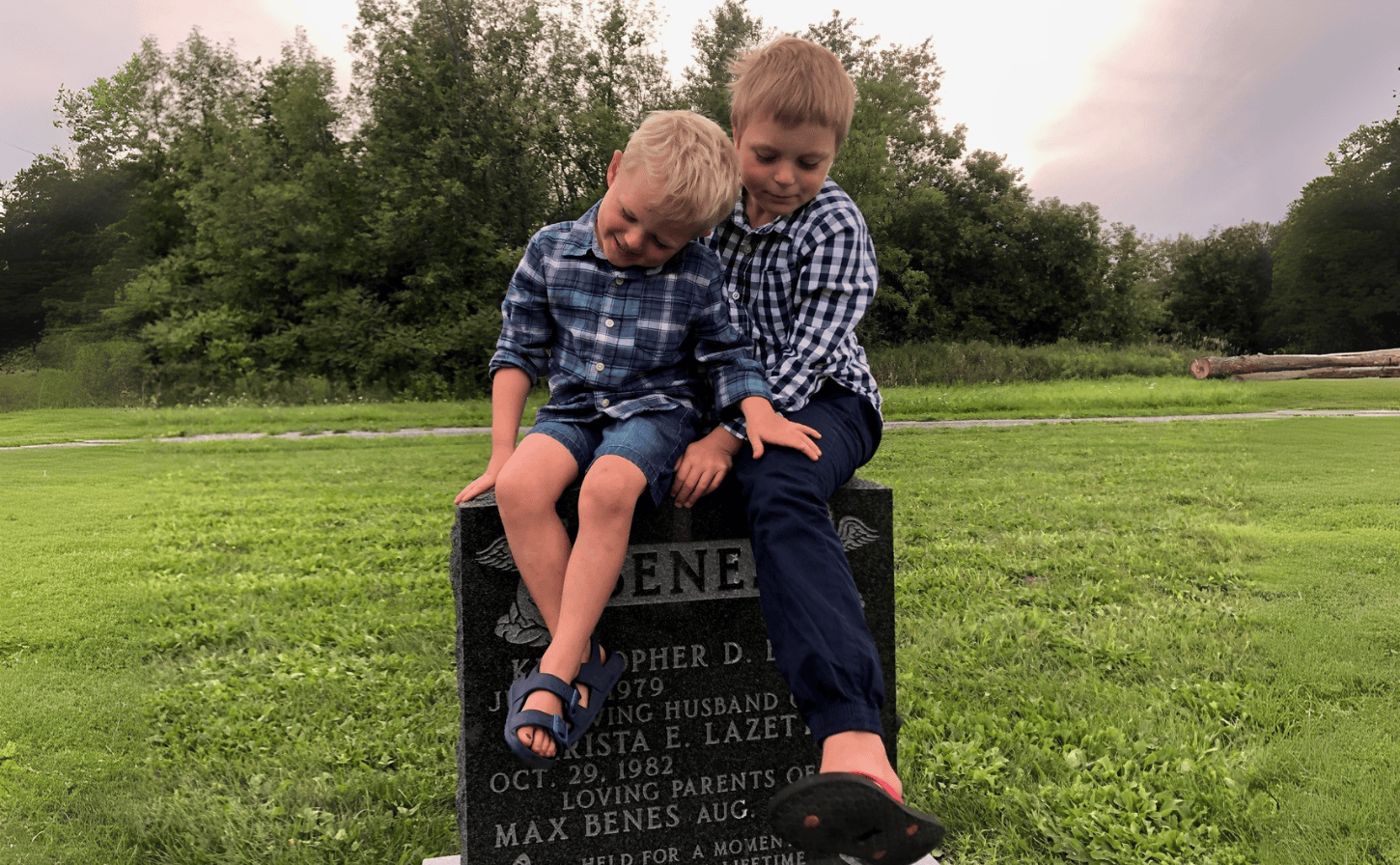
Big brothers Simon and Henry pay tribute to Max.

Krista Beneš recently made a career change as Manager of Prenatal Screening and Complex Perinatal Portfolio at the Better Outcomes Registry & Network (BORN).
Cherished memories
When I became pregnant again, with our son Simon, anxieties naturally arose. Along with physical concerns, there were also nagging worries like, ‘What if everyone forgets about Max?’
Henry helped alleviate that fear when he first took part in his school’s annual Terry Fox Run. Each student was given the chance to dedicate their run to someone, and Henry’s tribute card read, “Terry ran for me, I am running for Max.” I was so proud. Henry’s tribute made me think we must be doing something right, teaching our boys that they can remember their brother.
Other people remember Max, too. Loved ones still call or text me on his birthday. It means a lot. I’m not suggesting that everyone needs to do this, but the shared acknowledgement feels supportive to me.
With each passing year, our love for Max grows more layered, and his mattering in our family never wavers. Earlier this year, I saw a job posting that asked, “Are you passionate about improving the health outcomes for pregnant individuals and their babies?”
I felt this pull. I’d been at the Mental Health Commission of Canada for nine years and loved it, but who better to contribute to an understanding of how we could do this than someone who’s experienced the most devastating outcome of all?
Now, after taking a big professional leap, I’m surrounded by a team of incredibly bright, passionate individuals who are all working towards the vision of ensuring the best possible beginnings for lifelong health. What a great way to honour Max’s legacy.
As I languished during the isolation of the pandemic in March 2020, I was forced to live in the present.
 Moment of Impact, June 2020
Moment of Impact, June 2020
I was luckier than most when the global pandemic erupted in early 2020. I had a car, and I lived near the country. I was still deeply impacted by the necessary isolation, and as the weeks dragged on a sense of lethargy, maddening boredom and loneliness began to creep around me.
The snow soon thawed, and I took to my car for refuge. When I’m driving, even to 7/11 for snacks, it’s like I’m doing something, going somewhere. This illusion kept me grounded during a time where life seemed so desolate.
As the eerie stillness gnawed at me, my drives grew longer. I discovered places where I could sit, breathe, and observe nature. I noticed things as I drove, and soon I began to pull over when I saw something appealing, whipping out my phone and hopping out of the car while it was still running.
Spring bloomed into summer, and I spent my days driving listlessly and taking pictures. Slowly, my cameras accumulated in the passenger seat, and a new habit was born. My car and cameras became my closest companions, and I started to use photography to truly experience “living in the moment.”
The photos weren’t extraordinary –– a tree shrouded in the mist, its bare branches swaying; a bright orange sun reflected in a silent stream –– but I didn’t photograph these things because they were profound. They grounded me in the present, which was new to me.


I’m a planner. I need to know what’s next, to map every step forward meticulously. I’ll often enter a perfectly planned stage of my life without giving myself time to revel in my accomplishment before I start planning my next move.
That being said, the forced stagnancy imposed in 2020 stressed me out. Not knowing what was next, just not knowing made me tense and distracted.
Before, when I began taking photos more seriously, I’d photograph things in a clean-cut, symmetric sort of way. If there was a silhouette, I’d frame it in the centre. I required perfect days, and the photo would need to be what my eyes saw exactly, not creatively framed, or abstract at all. Once, my sister told me my photos looked like Google Image results, that if she searched a location photos like mine would appear, and that nothing about them was unique.
This annoyed me then, but now I get it. My photos were too poised, plastic even. Totally lacking in originality.
This period of my life enabled me to appreciate living near the country. Anytime the elements shifted, orienting themselves in a way that grabbed me, I’d head in the direction of that ephemeral muse. I began capturing moments with a transformed perspective and objective.


One morning, a fog blanketed the ground. I jumped in my car and drove deeper into the country, taking pictures of cows grazing, sprawling farmlands, birds swooping low over the river. I also did this during a lightning storm, after a heavy rainfall, and in the hour before sunset and sunrise nearly every day. I focused on what I could see, hear, and sometimes touch. I carried this new skill with me, and I genuinely believe that I am a better photographer and artist altogether.


When I had no future to predict or curate, I had the present. I had what was around me all along, and I’ve managed to immortalize it in a way I never could before. Instead of trying to capture something that seemed authentic, I began to take pictures of moments as they happened.
Now, as I adjust to my new normal –– living in a different city, embracing new experiences, meeting new people –– I can actually enjoy the present instead of trying to predict the future.
The anxiety about the future is still there, but it’s dulled by the realization that one day the future will be the present and I’ll have been busy making the most of it, cultivating perspective which will benefit me today and forever.
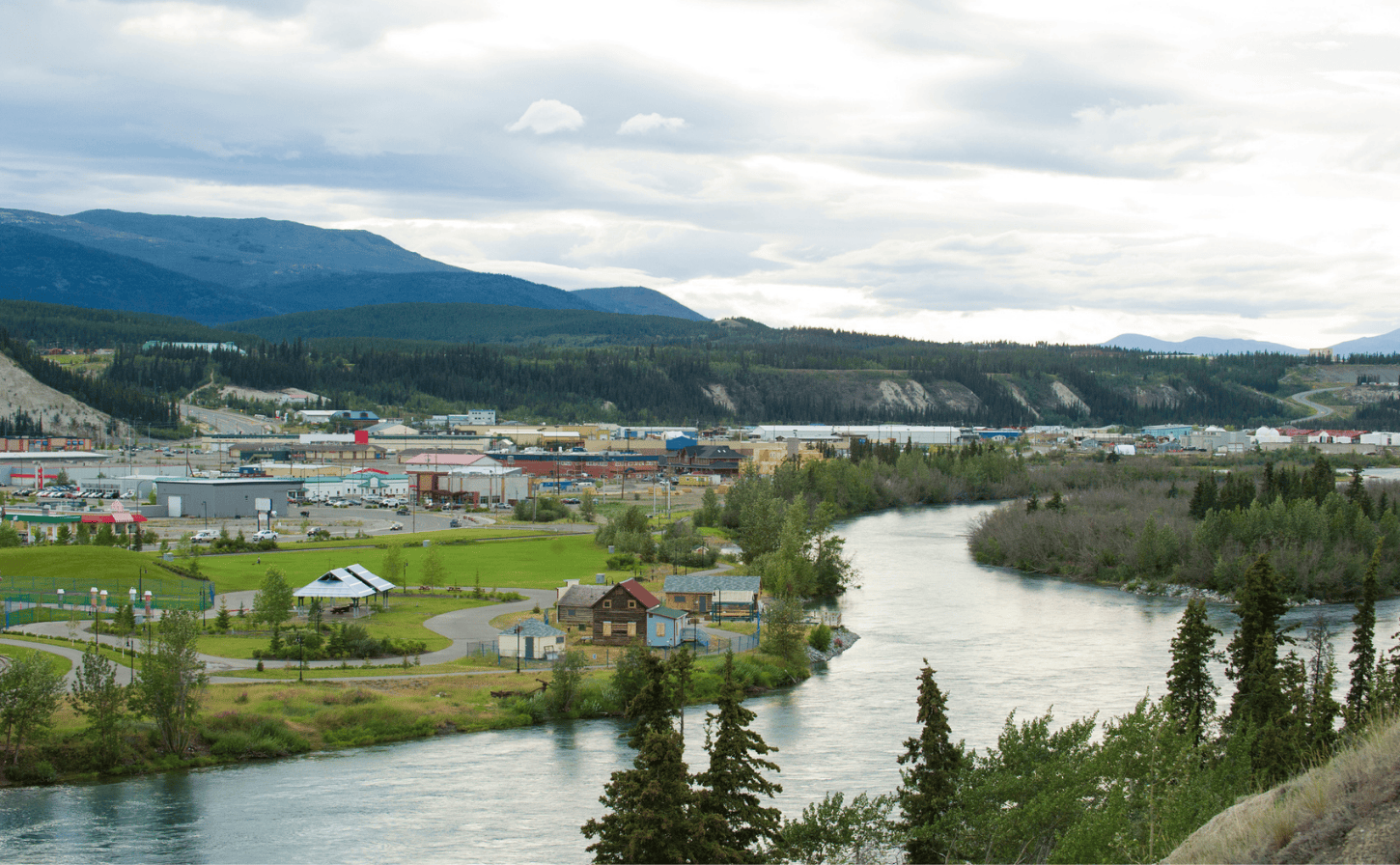
Whitehorse along the Yukon River. Photo: AscentXmedia.

Taryn Ellens founded Ainome – pronounced “I know me” to support self-determined strategies for mental health and wellness in Indigenous communities. Photo: Manu Keggenhoff.
New approaches to therapy
A shift in approach is one way of adopting and adapting mental health in Indigenous communities; another is improving access through online resources, which can make a difference between having and not having care, particularly in geographically remote communities. Virtual counselling was very appealing to Colbi Mike; it was the first place she looked when searching for a new therapist.
Mike was looking for a way to bridge cultural teachings from her Indigenous background with standard mental health approaches. The 27-year-old is from Poundmaker Cree Nation in Saskatchewan and is the first generation in her family to grow up outside of the residential school system. Mike sits on the Youth Council of the Mental Health Commission of Canada, offering insights on addressing barriers to maternal mental health and the effects of oppression on Indigenous peoples.
“I grew up with different teachings – go to Elders, do ceremony, be with family,” Mike says. “So, when I first started seeing a therapist when I was very young, it felt like an internal struggle, like I was betraying someone,” she says. She started to move from in-person to online therapy to find an approach that would meet her needs. She says it took a bit of work to ensure the services would be covered under her health plan, and the get-to-know-you sessions felt a bit slow. However, once things ramped up, Mike felt that she hit a stride with her current practitioner.
“We had a lot to say to each other,” she says. “I’m an info-intake person, and my therapist is willing to share her personal experience in connection with mine, as she has children too.”
Online therapy offers other opportunities, Mike notes. “Being in the comfort of my own home, I’m able to smudge,” she says. “Having a space that I’m able to cleanse myself, before and after therapy, has been really important to me.”
As practitioners and organizations seek to improve access to mental health, considerations are being made for data sovereignty, online safety, and culturally appropriate care, while also considering what innovations are possible, such as through the work of Ainome and other startups, that make space for culture and connection.
It’s a chance to imagine better, Ellens says. “Ainome was born from frustration with existing systems that weren’t telling the full story around mental wellness and Indigenous self-determination, and with the hope that we could use technology in ways that heal rather than harm. Our work is about co-creating tools that reflect lived experience and community-led definitions of care.”

Kathy Bates stars as the brilliant septuagenarian Madeline Matlock in drama series, MATLOCK, inspired by the classic television series of the same name. Madeline achieved success in her younger years and decides to rejoin the work force at a prestigious law firm, where she uses her unassuming demeanor and wily tactics to win cases and expose corruption from within. Photo: Brooke Palmer/CBS via Getty Images.
Who turned on the cloaking device?
For this reason, Dr. Susan Braedley, Professor at Carleton University’s School of Social Work, says that, after fifteen years of studying long-term care and age-friendly communities in national and international research projects, one of her teams’ key findings is that inclusivity must guide the planning and designing for care homes, retirement communities, and programming for older adults.
“We’ve seen a lot of promising practices,” says Dr. Braedley. “And then we’ve seen some things to avoid, things that caused great distress to older adults.”
For example, she recalls a day program designed for people with mild cognitive impairment in a Canadian community where many residents’ first language was Mandarin. Personal support workers didn’t speak Mandarin, and the activities all assumed that participants were familiar with mainstream Canadian customs and holidays.
“If you think you’re supposed to know the answers but don’t, it can be really confusing, because you start to think your memory is worse than it is,” Dr. Braedley explains. “The program produced a lot of anxiety. It was supposed to reduce social isolation for people living with dementia and, actually, I think it was having the opposite effect. Cut-and-paste programs don’t work.”
It’s not all bad news, though. In the course of her research, Dr. Braedley observed scores of programs that were culturally appropriate, community-based, and well-designed for the actual participants. And, in those spaces, Dr. Braedley witnessed and, herself, felt, a lot of joy. One of her many favourites was a program offered at the 519, a non-profit agency in Toronto that serves 2SLGBTQI+ communities. This program matched younger volunteers from the community with older adults experiencing loneliness.
“The older people had amazing experiences, sometimes just by having someone to help them negotiate the city when they were feeling uncertain about being out on their own,” she says. “But what was so interesting is that many of the younger people were working remotely and were saying, ‘We’re lonely, too. We’re isolated’.”
Eddy Elmer, a Vancouver gerontologist and research consultant specializing in aging and mental health, says that older people from 2SLGBTQI+ communities are far more likely to be socially isolated and lonely.
“Some of it’s just because it’s a smaller population base, so it’s harder to meet people or find a partner,” says Elmer. “LGBT people over the age of 70 also grew up at a time when being gay was highly stigmatized. It was illegal, it was criminalized, and it was pathologized, so they’re more afraid of being rejected and discriminated against.”
Elmer fears that we’re taking steps backwards now, with changes in our online climate, and a general rise in anti-2SLGBTQI+ sentiment. As such, he warns that risks are on the rise, particularly for transgender older adults.
The mysterious case of the vanishing older adult
Older people experiencing income insecurity, homelessness, incarceration, or pre-existing depression all tend to be more vulnerable, as are older men who have recently experienced a life transition, such as retirement. Some attribute this to the fact that, broadly speaking, women have larger social networks. When men stop working, by contrast, many lose their most important social space.
For many, though, it’s also about a shift in self-perception and a loss of identity.
“People are saying to me, ‘I was a high school principal, or a professor, or a lawyer and I had all these different roles and identities’,” says Dr. Raza Mirza, Director, National Partnerships for HelpAge Canada. “And then they retire, and their perception is that ‘Now all I’m seen as is as an older person and we’re all kind of lumped into this one big group. That’s my identity now’.”
One of Mirza’s many research projects aimed at helping older adults is a study with Men’s Sheds Canada of called “Men’s Sheds,” a program designed to help people establish new roles as mentors in society and connect and engage with other men of all ages.
“The idea is to empower older men,” he says. “It’s also about health promotion, though, because they can talk to one another through life transitions, share resources and share information that impacts the mental and physical well-being of older men.”
That could have a serious impact given that, simple preventative measures and screening can make a big difference when it comes to the social, mental, and physical health of older adults. Hearing aids and eyeglasses, for example, are a low-intervention way to reduce social isolation and improve well-being.
“Sensory loss is very important because many older adults have hearing or vision problems,” says Dr. Fereshteh Mehrabi, post-doctoral research fellow in Concordia University’s department of psychology. “Dramatic hearing loss is much more prevalent among men than women and, often, they choose not to even try to communicate of socialize at all because it seems like too much of a bother, which can contribute to frailty over time, as reduced communication and social engagement may lead to physical decline and isolation.”
Seen, heard, and invited to the party
There’s some debate about why older men experience hearing loss, but there’s little doubt as to why many older men don’t want to use a hearing aid, namely, because that’s associated with older people. In other words, people often choose to withdraw from the world rather than deal with age stigma. (Incidentally, the new generation of hearing aids are far more discreet, and the tech allows users to do neat things like tune out ambient noise to focus on the person speaking, which, if you think about it, sounds like a good superpower to have).
Older women aren’t immune to hearing problems, but, by the numbers, Mehrabi says that, for women, screening for and preventing frailty should be the top priority. Women are far more likely to experience frailty than men and her recent study, published in Age and Ageing found that, over a long-term period, frailty leads to social isolation and loneliness, perhaps for the simple reason that it’s harder to go out and join in social and physical activities. It doesn’t help that, even though women’s fitness is a massive growth industry, there are plenty of cultural and systemic barriers keeping older women from building muscle with good diets and resistance exercises.
“The perfect neoliberal older person has enough money to last them the rest of their life and is using their Fitbit to keep them active and healthy,” says Dr. Braedley. “The idea is that we have so much control and we can keep ourselves healthy if we eat right and do all the good things. Which is ridiculous because we all die.”
“Many, many people, and disproportionately women, don’t fall into that model of the perfect, self-reliant, older person,” she adds. “So, I think it’s about that. I think it’s about classism, sexism, racism, and ableism all combined.”
Back to those invisible women, it’s important to note that it can feel like a superpower for some, but it’s damaging to others. “The older person who feels invisible and comes from a marginalized background will not see being invisible as having any sort of benefit,” says Flett. “For folks experiencing co-occurring injustice, inequity and invisibility, that’s a very painful combination.”
That makes it everyone’s responsibility to find a way to make people secure in the knowledge that they matter—no matter what their age.
Older adults are more likely to suffer from social isolation. Loneliness is increasingly being recognized as being bad for our health. The good news is that mattering and belonging can flip the script. Our series explores these and other related concepts.
“I think I was 50 the first time a younger person in the office asked me when I was going to retire,” recalls Pamela, a 62-year-old government employee who lives in Edmonton. “He said it was high time people like me got out of the way to make room for people like him.”
Pamela, a pseudonym to protect her identity, has worked for the same department since the mid-1990s. She’s qualified, knows all the ins and outs and, according to her, actually trained her last two bosses for roles she applied for. She never even got an interview. She recently filed a workplace discrimination complaint against her employer, because she believes she’s the victim of ageism.
“Being constantly passed over for promotions is frustrating,” says Pamela. “Worse than that, though, is being made to feel like you’re a burden.”

Dr. Alison Chasteen, a social psychologist at the University of Toronto.
Pamela isn’t alone. A recent Employment and Social Development Canada survey found that almost half of respondents 55 or older felt they had experienced ageism, a form of discrimination that the World Health Organization says is one of the “most socially normalized.” Not only is age stigma prevalent, but it can also damage older adults’ abilities, says Dr. Alison Chasteen, a social psychologist at the University of Toronto.
“If you activate negative stereotypes in older peoples’ minds, that can elevate a cardiovascular stress response that can also affect memory function, so they don’t do as well on, say, a free recall test where you have to recall a list of items,” says Dr. Chasteen, noting that it’s also been shown to impact motor function.
Fixed mindsets
Internalizing negative stereotypes to the point that they feel like they define our characters isn’t unique to older adults experiencing ageism. Self-stigmatization is a common phenomenon that runs across all forms of stigma but, when it comes to ageism, there’s another layer, because older adults may, themselves, have held negative ideas about ageing when they were younger.
Given how pervasive and complicated age stigma is, an essential first step in tackling it is to stop using terms that carry negative connotations, such as “the aged,” “old-old,” “senior citizens” and “the elderly.” These imply a fixed identity and/or evoke images of frailty. By contrast, the term “older adult” reminds us that age is relative and ever-changing.
“Really what we’re talking about here is ageism,” says Katie Ellis, Program Manager at the Mental Health Commission of Canada, who recently led a research project on mental health and older adults in Canada. “Using language with negative associations really does have a negative impact on quality of life, because stigma can stop people from thinking they can get better access to care or participate in certain activities.”
Stigma and social exclusion go hand in hand. Pamela says that, even though she’s resisting the push for her to quietly retire from her life-long career, she’s often left out of after-work gatherings and finds that holiday parties can be awkward because she’s not in the cool kid crowd. She’s lucky to have good friends outside of work, but it’s easy to see why age stigma is closely associated with mood disorders, diminished well-being, and feeling less inclined to seek medical treatment, as well as loneliness and social isolation.

Mental Health Commission of Canada program manager Katie Ellis led a research project on older adults and mental health. Stigma can lead to a negative impact on quality of life.
Mattering and belonging – what’s the difference?
“I think the big thing with discrimination and prejudice and stigma is that you’re no longer seen as a unique person with valued attributes,” says Gordon Flett, Honorary President of the Canadian Psychological Association 2024-2025 and former York University Canada Research Chair. “A key element of ‘mattering’ is just being seen as an individual with valued attributes and, instead, you’re seen according to a prescribed box that you’re put into, and you feel unvalued or devalued.”
“Mattering” shares a lot of space with the idea of “belonging” but takes it a step further. It’s possible to belong to a club but still feel unimportant. Mattering means that people value your contributions and, simply enough, you matter. That sense of purpose and meaning seems to offer protective qualities, since it’s correlated with resilience and better health outcomes. Anti-mattering, on the other hand, is closely associated with discrimination and stigma.
“Anti-mattering is so destructive because it means treating people like they’re insignificant or invisible or unseen, unheard and unvalued,” Flett explains.
It’s hard to get people to see beyond stereotypes if you rarely, if ever, interact with people outside of your generation, though. Few Canadians do, since “age bubbles” define a lot of peoples’ social lives. As ageist as some workplaces may be, it’s not uncommon for people from different generations to work on projects together on the job site. By contrast, many social spaces are often tightly age-segregated in ways we don’t always even notice.
“I went to a wedding with my sister and my mother recently and we expected to spend the evening together,” says Dr. Raza Mirza, Director, National Partnerships for HelpAge Canada. “But my mother was sat at a table with older adults, and I was sat at a table with younger people who I didn’t have anything in common with. I would have far preferred to sit with my mother.”
The assumption that older adults only want to talk to people their own age is particularly striking to Mirza, whose career is focused on fighting age segregation through intergenerational projects. Although many are in their infancy, there are a lot of pretty cool projects aimed at getting people out of their age bubbles.
In Alberta, the Canadian Alliance for Intergenerational Living launched a pilot project last year that placed students looking for affordable housing into retirement communities in exchange for leading classes in, say, art, scholarship, or fitness.
St. Lawrence, a school in Champlain, Quebec, arranges intergenerational living situations by offering students two meals a day and free lodging in a residence for older adults in exchange for 10 hours of volunteer work in the home per week.
Vancouver’s Volunteer Grandparents has a “Family Match” program that sees older adults sign up to help mentor kids whose biological grandparents can’t play active roles in their lives. Ontario resident Heather Walker wanted to take part in the program but was too far away, so they made her a pen pal to a 15-year-old.
“She seemed like a younger me,” says Walker, who will celebrate her 70th birthday this summer. “Her passions were writing, and social justice and I had so many questions, my letter back was five pages long.”
Now she has a new role as a pen pal with an entire class in an elementary school. She helps them with things like sentence structure and sends them Valentine’s Day cards and other special treats.
Burst your bubble
One of the better-known age bubble-bursting projects is Raza Mirza’s “Intergenerational Classroom,” an initiative that sees a third-year University of Toronto Ageing and Health class pop up in a common room at Christie Gardens, a Toronto retirement community and long-term care home. Students and residents take the class together for the entire semester.
“It’s been highly, highly successful, because we facilitated a platform where people can feel valued,” says Mirza. “We keep hearing that people felt they had a role, felt that their contributions were meaningful, and felt a sense of belonging. But there was also reciprocity, so it wasn’t this older person who was just the recipient of information or sharing information. There was this back-and-forth exchange.”
Nobody gets stuck in the corner at the kids’ table, either. Everyone has a chance to break out of their age bubble and get to be seen as a unique person. It’s a fabulous model showing a path forward for us to fight against stigma, negative stereotypes, and anti-mattering. And, in fact, it might even help people re-define what “being old” means.
“We’ll start the class by asking the students, ‘At what age do you think a person is old?’,” says Mirza. “People say things like 40 or 50 or 60. Then, after being in the class and listening to older adults for 12 weeks we ask them the question again. They say things like, ‘I’m not sure’ or ‘I think old is a perception or a feeling.’ They focus on the similarities they have and the things that they have in common,” he adds. “They don’t focus on the age difference anymore.”
Older adults are more likely to suffer from social isolation and loneliness is increasingly being recognized as being bad for our health. The good news is that mattering and belonging can flip the script. Our series explores these and other related concepts.
When Pat Flude was experiencing painful side effects during her breast cancer treatment, a doctor from the pain clinic at Toronto’s Princess Margaret Hospital (PMH) gave her a “social prescription” for a mindfulness-based cognitive behavioural therapy class.
“I went every week for about three months,” says Flude, a 78-year-old retired teacher and cancer survivor. “The psychiatrist who led the program, Dr. Mary Elliott, was marvelous. It was so excellent; I even did a follow-up class in loving kindness.”
Since everyone in the class was also being treated for cancer, there was a real sense of community. Flude says she looked forward to the reunions that took place at quarterly graduate sessions. “For me, at that time,” she recalls, “it was really life’s blood.”
Although not every hospital is as proactive as PMH at offering prescriptions for things other than drugs, the “social prescribing” movement is growing by leaps and bounds. The guiding principle is to address the social determinants of health – non-medical factors that influence health outcomes – that are often neglected in medical settings. To fill that gap, primary health care providers refer a patient to a senior resource coordinator who steps in to “prescribe” wellness opportunities (specifically chosen classes or outings based on interest) often for older adults who have higher rates of being at-risk for loneliness and/or social isolation.
From isolation to inclusion
“The big one is social connection,” says Connie Newman, executive director of the Manitoba Association of Senior Communities. “We’ve got some older adults who haven’t been out of their apartments for too long. With a social prescription, we can connect them to one of Manitoba’s many older adult groups.
“Some might be at the local legion; in other communities, it could be the local senor centre,” Newman explains. “Wherever it is, the clients sometimes need a little support to join.”

Connie Newman, executive director of the Manitoba Association of Senior Communities: Social prescribing can open the door to connecting older adults to others in their communities.
Although research associating social isolation and loneliness with negative health outcomes began, in earnest, a little more than 40 years ago, programs to prevent or reverse these conditions and foster a feeling of belonging are relatively new. Spurred, in part, by the pandemic, which raised awareness of negative mental health effects associated with isolation, “social health” (well-being as an outgrowth of social connection), has become a hot topic lately. Japan and the United Kingdom both have ministries devoted to addressing loneliness, which some consider an epidemic, especially among older adults.
Here in Canada, the Canadian Coalition for Seniors’ Mental Health has recently launched the world’s first clinical guidelines for addressing social isolation and loneliness. Since older adults experiencing isolation often see health and social service professionals, clinicians are key people for identifying at-risk patients, so it’s very important to get them on board.
“Although there’s been a huge amount of research in the area focused on associated health risks there has been relatively little written from the perspective of how to actually help people,” says Dr. David Conn, a geriatric psychiatrist who works at Baycrest Health Sciences and the University of Toronto.
The guidelines, which are making their way into healthcare and community settings, are designed to help clinicians screen for loneliness and isolation, assess the problem and its causes and make helpful recommendations. In some cases, a social prescription might transform the quality of life of a person experiencing isolation but, for those with chronic loneliness, recovering from those feelings is often much more complicated. Neuroscientists have even suggested that loneliness can re-shape the brain in ways that make social contact less rewarding, thereby making it harder—but not impossible—to “cure” loneliness. A meta-analysis of research found that a range of therapies including animal therapy, exercise, and cognitive behavioural therapy were associated with reduced feelings of loneliness in older adults.
The power of place in fostering connection
That’s a nugget of good news but, as we should all know at this point, prevention is, by far, the best intervention. Some researchers advocate for social prescriptions for people of all generations, as well as working to remove health equity barriers, so that we have a population that’s in good health as it moves into middle age. As Dr. Conn points out, problems with depression, hearing, vision, mobility, and chronic pain can impact our capacity for socializing and staying active.
Providing an environment for people to stay fit and connected to the community goes far beyond healthcare and even public health, since it involves reimagining a range of public spaces, some of which we take for granted. Over the past 20 or more years, we’ve heard a lot about the “third place”—spaces like barber shops, cafés, and shopping malls that are neither work nor home but can foster community and a sense of belonging. The next frontier may well be “fourth place”—streets, squares, bus stops—which, if well-designed, can help promote social health and cohesion. That can only work if they’re truly accessible, however.
“The design is often good in a privileged neighbourhood,” says Julie Karmann, PhD candidate at the University of Montreal’s School of Public Health. “But if you go into a more deprived neighbourhood, you can see that the street is no longer that accessible and not that pleasant for walking.”
Karmann’s work is based in the idea that the simple act of walking can help social health, of which connectedness is an important component. Even relatively well-designed fourth places, though, often miss the mark when it comes to being truly age-friendly.
“Basic improvements like more accessible and affordable transit, safer intersections, and well-maintained sidewalks are essential,” says Eddy Elmer, a Vancouver gerontologist and research consultant specializing in aging and mental health. “People don’t want to go outside if the streets are dark or feel unsafe, regardless of age, but this is especially true for older adults who worry about slipping, falling, or other hazards.”
Maintenance, regular snow and ice clearing, as well as accommodations for persons with disabilities should seem like a bare minimum, but austerity measures in various municipalities have often led to worsening conditions. While we wait for political change, social health programs such as prescriptions can help, especially the ones that move beyond the individual and involve the community.
More walks, more smiles
“One of my favourite programs is from the Netherlands, which has a whole strategy and campaign against loneliness,” says Conn. “One of the programs is an app that connects older people who don’t have a pet with a younger person who has a dog but doesn’t have enough time to walk the dog because they’re out working all day long. It has many benefits for all involved including the dogs!”
Burnaby B.C.’s “Say Hello” campaign is arguably even more effortless. Initiated in 2020 by local physicians worried about pandemic-induced social isolation and loneliness, the project encouraged folks to be a little friendlier to the people they passed on the street.
“It’s super simple, but yet requires a whole paradigm shift, because it has nothing to do with a physician or a clinic,” says Karmann. “Just implementing the norms of greeting in the neighbourhood or smiling to the person you meet in the street can make a huge difference with your sense of belonging.”
Karmann says it’s a tiny gesture that can have a big impact on the population, not just the individual.
“It’s just knowing the people around you,” she adds. “It can be as easy as asking, ‘How are you doing?’.

Vancouver gerontologist Eddy Elmer: You can be isolated and not lonely; you can also have a wide social circle and still feel lonely. It all depends on one’s needs and expectations.
Mattering is good for the grey matter
Even though way fewer sabre-toothed predators are prowling around these days, being a member of a clan is still the safer and healthier choice for most people. A recent study from Carleton University found that higher belongingness is connected to better health outcomes for people of all ages—but particularly for older adults.
“What we found was that older individuals who felt they belonged to their neighbourhood were about six or seven percent healthier than people who didn’t,” says Mehdi Ammi, Associate Professor at Carleton’s School of Public Policy and Administration. “Belonging reduced most chronic conditions and was preventative in arthritis and anything connected to chronic stress.”
Social psychology proposes that high levels of belonging can help chronic stress, so it may offer a protective benefit to folks who feel like they have a place at the table. Though some positive psychologists say that while belonging is a good start, an even stronger protective benefit can be seen in people who feel like they matter.
“Belonging is fitting in and having a place,” explains Gordon Flett, Honorary President of the Canadian Psychological Association 2024-2025 and former York University Canada Research Chair. “Mattering is feeling a sense of significance and value within that place. For example, a person could be part of a community, but still feel they’re not being taken seriously.”
The correlation between loneliness and the feeling of not mattering is very robust, he says. “The research about loneliness and the elderly show that there are just too many people who don’t have any meaningful engagement of a prolonged nature with the people who matter to them,” Flett continues. “And they’re left to feel lonely. And when people feel alone and insignificant at the same time, we call that ‘double jeopardy’.”
Conversely, mattering is thought to provide a buffer of sorts that protects individuals from significant stress, whether it’s caused by loneliness, caregiving, loss of independence, and even financial issues.
“The bottom line is that knowing people value and care about you is very comforting,” says Flett. “And I think it also means that you’ll be more likely to ask people for help when you need it.”
It can be difficult for older adults to feel valued and have a sense of meaning, especially in North America, where the culture valorizes youth, fails to provide age-inclusive spaces or age-friendly cities, and views health as an individual responsibility as opposed to a collective one. All these things are factors in widespread loneliness amongst Canada’s older adult population.
While we wait for societal changes, many older adults who have the ability are finding ways of aging in community and generating mattering experiences for themselves. For some, that might be grandparenting. For others, it might be volunteering to help other older adults.
“My wife’s uncle Derek, who almost made it to 100 and lived by himself his whole life in Fort Qu’Appelle, Saskatchewan, was well-known for his volunteer work,” Flett offers. “He delivered Meals on Wheels to people younger than him into his 90s because he was in great shape.
“I once asked him if he ever felt lonely and he cut me off. He said, ‘Not for a second. Because I know there’s people out there who care. And I can get to them, and they can get to me’.”